What exactly does it mean to live in poverty? Although this is a heavily nuanced question, breaking it down from the perspective of a religious and educational institution is a key component of Catholic Social Teaching. In particular, when it comes to issues of health, the pillar of a “Preferential Option for the Poor and Vulnerable” does an excellent job addressing the issues of healthcare access and quality that manifest as a result of poverty. From this tenant, our faith calls us to always place the needs of the poor first. At the Second Vatican Council on December 7th, 1965, Pope Paul VI called for exactly this when he proclaimed that we must feed the people dying of hunger, for if we do not, we are killing them. Although his statement literally speaks of feeding the poor, Pope Paul VI was actually calling for preferential options for the poor across all facets of life, including health. However, if we are to create a preferential option for the poor, it is necessary to first consider WHAT it means to be impoverished of healthcare before determining HOW this issue can be rectified.
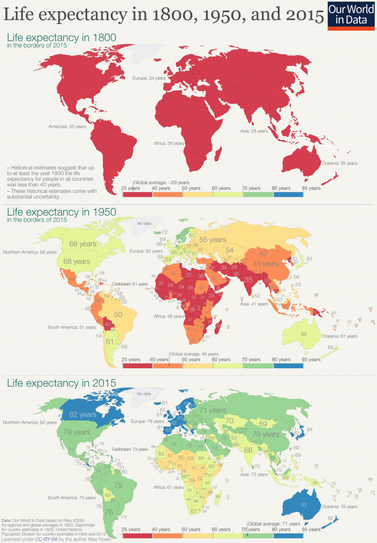
Taking a step back to examine the health of the human race as a whole, the question of “what is poverty” becomes a far more difficult one to answer. On one hand, humanity currently lives within a golden era of achievement which has brought about massive increases in overall quality of life. For example, a dangerous multi-week long journey that was once undertaken by foot can now be completed rather comfortably and in a matter of hours through aeronautical travel. Furthermore, through the groundbreaking strides in bioscience and technology that have taken place over the past 200 years, humans are living longer and healthier than ever before. In this time, average global life expectancy has risen from 29 to an astounding 71 years, vaccines have all but eradicated debilitating childhood diseases, cheap and accessible water sanitation has entered into the mainstream, and improvements in agrarian techniques have yielded far greater quantities and quality of food. From these arguments alone it can be easy to don a pair of rose-colored glasses and see the world for all the good that it contains; however, by doing so, we ignore the fact that reality is far more complicated than what is presented in this brief snapshot.
Taking a step back to examine the health of the human race as a whole, the question of “what is poverty” becomes a far more difficult one to answer. On one hand, humanity currently lives within a golden era of achievement which has brought about massive increases in overall quality of life. For example, a dangerous multi-week long journey that was once undertaken by foot can now be completed rather comfortably and in a matter of hours through aeronautical travel. Furthermore, through the groundbreaking strides in bioscience and technology that have taken place over the past 200 years, humans are living longer and healthier than ever before. In this time, average global life expectancy has risen from 29 to an astounding 71 years, vaccines have all but eradicated debilitating childhood diseases, cheap and accessible water sanitation has entered into the mainstream, and improvements in agrarian techniques have yielded far greater quantities and quality of food. From these arguments alone it can be easy to don a pair of rose-colored glasses and see the world for all the good that it contains; however, by doing so, we ignore the fact that reality is far more complicated than what is presented in this brief snapshot.
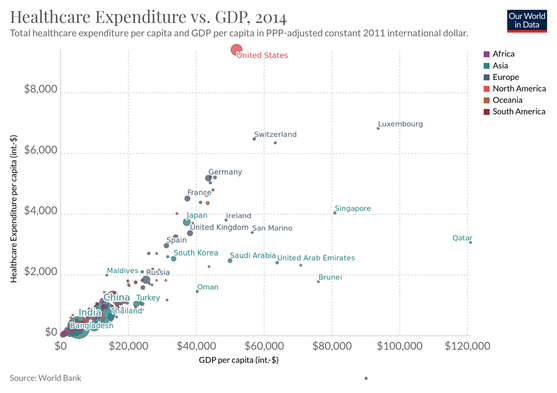
Even though we have seen the extent of these improvements stretch across the face of the Earth, they have not done so in an equitable manner. One of the poorest regions in the world, sub-Saharan Africa, continues to face extreme levels of poverty with millions of people making less than $1.90 per day based on data provided by the Institute for Security Studies. Furthermore, these deeply impoverished countries struggle with crippling amounts of debt, government corruption, and international trade deficits that have cemented their multi-decade long statuses in poverty. Taken together, these factors have had devastating consequences for the health of the people who live in these areas. A 2009 study undertaken by the US National Research Council found that sub-Saharan Africa, as an entire region, spent an average of 6.1% of its annual GDP on healthcare expenditures. This stands in vast contrast to the 9.5% spent, on average, by the 37 member countries that constitute the Organization for Economic Cooperation and Development (OECD). On a per-capita basis, low-income countries within sub-Saharan Africa spent about $25 per person as opposed to the $4,600 spent per person by OECD nations. As a testament to these massive inequalities, it is estimated 1 out of every 14 adults in Africa (7.14%) are infected with the human immunodeficiency virus (HIV), a far greater fractional percentage of the population than most other regions of the globe. Even in high-income countries such as the United States of America where healthcare spending is relatively large on a per capita basis, healthcare is far from perfect. According to data provided by the Brookings Institution, health expenditures in the U.S. nearly quadrupled from 1980 to 2018 while the supply of physicians entering the job market remained relatively constant leading to widespread shortages and increased costs. These factors, among many others, have been key players in the healthcare crisis that we are currently muddling our way through despite our status as one of the wealthiest countries on Earth. As disappointing as it may seem, the data loudly highlights how the poor, regardless of geographical location, suffer when it comes to attaining adequate care. At an initial glance, it may seem logical to attempt to solve these issues by creating safety net programs or throwing money at impoverished nations in the form of debt relief. If money talks, why can’t it then be leveraged to abruptly reverse the lapses in healthcare access and quality that we see all over the world? For one thing, shotgunning wads of cash at a deeply systemic issue are by no means guaranteed to have any positive and/or lasting ramifications. If weak infrastructure or damaged healthcare systems hinder the intended effects of monetary relief, a more strategic plan is not only wise but necessary.
Healthcare policy research put forth by The School of Public Health at the University of the Western Cape has advocated for the need to take on alternative angles to solving issues underlying poverty of healthcare. The centerpiece of their call to address these widespread issues involve strengthening the community base of healthcare by greatly increasing primary care initiatives. The authors argue that the current focus on tertiary care centers does a great disservice to the vast majority of people who require basic primary care since these institutions typically benefit the upper echelons of society. By mobilizing more individuals to enter into basic healthcare services, a much greater proportion of the population will gain access to adequate and affordable healthcare. The main theme of this boils down to how stronger primary care facilities allow communities and local governments to sustain themselves and address the needs of their own populations on a smaller and more controlled scale.
At the end of the day, there is no easy answer to addressing the elusive and multi-layered issue that underlies healthcare inequality. These divisions exist in almost all areas of life and always have since the beginning of time. There is no one right answer to these challenges nor one quick fix that will address these issues overnight. However, the doctrines set forth by CST compel us to consider our faith and the basic values of Catholicism that focuses on respecting the dignity and humanity of our fellow man. By empowering our individual communities to address the healthcare issues faced by society’s most vulnerable, we ultimately create a preferential option for the poor that fulfill CST’s call for us to serve our fellow man.
Published By: Jake Berg
Healthcare policy research put forth by The School of Public Health at the University of the Western Cape has advocated for the need to take on alternative angles to solving issues underlying poverty of healthcare. The centerpiece of their call to address these widespread issues involve strengthening the community base of healthcare by greatly increasing primary care initiatives. The authors argue that the current focus on tertiary care centers does a great disservice to the vast majority of people who require basic primary care since these institutions typically benefit the upper echelons of society. By mobilizing more individuals to enter into basic healthcare services, a much greater proportion of the population will gain access to adequate and affordable healthcare. The main theme of this boils down to how stronger primary care facilities allow communities and local governments to sustain themselves and address the needs of their own populations on a smaller and more controlled scale.
At the end of the day, there is no easy answer to addressing the elusive and multi-layered issue that underlies healthcare inequality. These divisions exist in almost all areas of life and always have since the beginning of time. There is no one right answer to these challenges nor one quick fix that will address these issues overnight. However, the doctrines set forth by CST compel us to consider our faith and the basic values of Catholicism that focuses on respecting the dignity and humanity of our fellow man. By empowering our individual communities to address the healthcare issues faced by society’s most vulnerable, we ultimately create a preferential option for the poor that fulfill CST’s call for us to serve our fellow man.
Published By: Jake Berg
